Why Is Interoperability Important in Healthcare During Crises?
 Iron Bridge
Iron Bridge

In a public health emergency, time is critical. Sharing patient data among hospitals, pharmacies, laboratories, and government agencies can help contain an outbreak before it escalates. This is why interoperability is essential in healthcare, particularly during pandemics, vaccine rollouts, and emergency planning.
When systems are connected, public health officials gain real-time visibility, and that visibility saves lives.
The COVID-19 pandemic made this clear. It also exposed how far the U.S. healthcare system still must go.
How Disconnected Systems Slow Emergency Response
Most healthcare organizations operate multiple data platforms, each serving a different purpose and following different standards. Hospitals use one system, pharmacies another, and public health departments often rely on legacy technology that does not communicate with either.
During a crisis, those communication gaps become dangerous. A hospital may be unable to quickly report new cases to a state health department because its EHR formats data differently. A pharmacy may administer a vaccine but fail to transmit that record to the state immunization registry for days. These challenges are not theoretical.
According to MMWR, the first confirmed COVID-19 case in the United States was reported on January 21, 2020. Although the outbreak initially appeared contained, it spread rapidly through February and April. Disconnected systems created blind spots at the worst possible time.
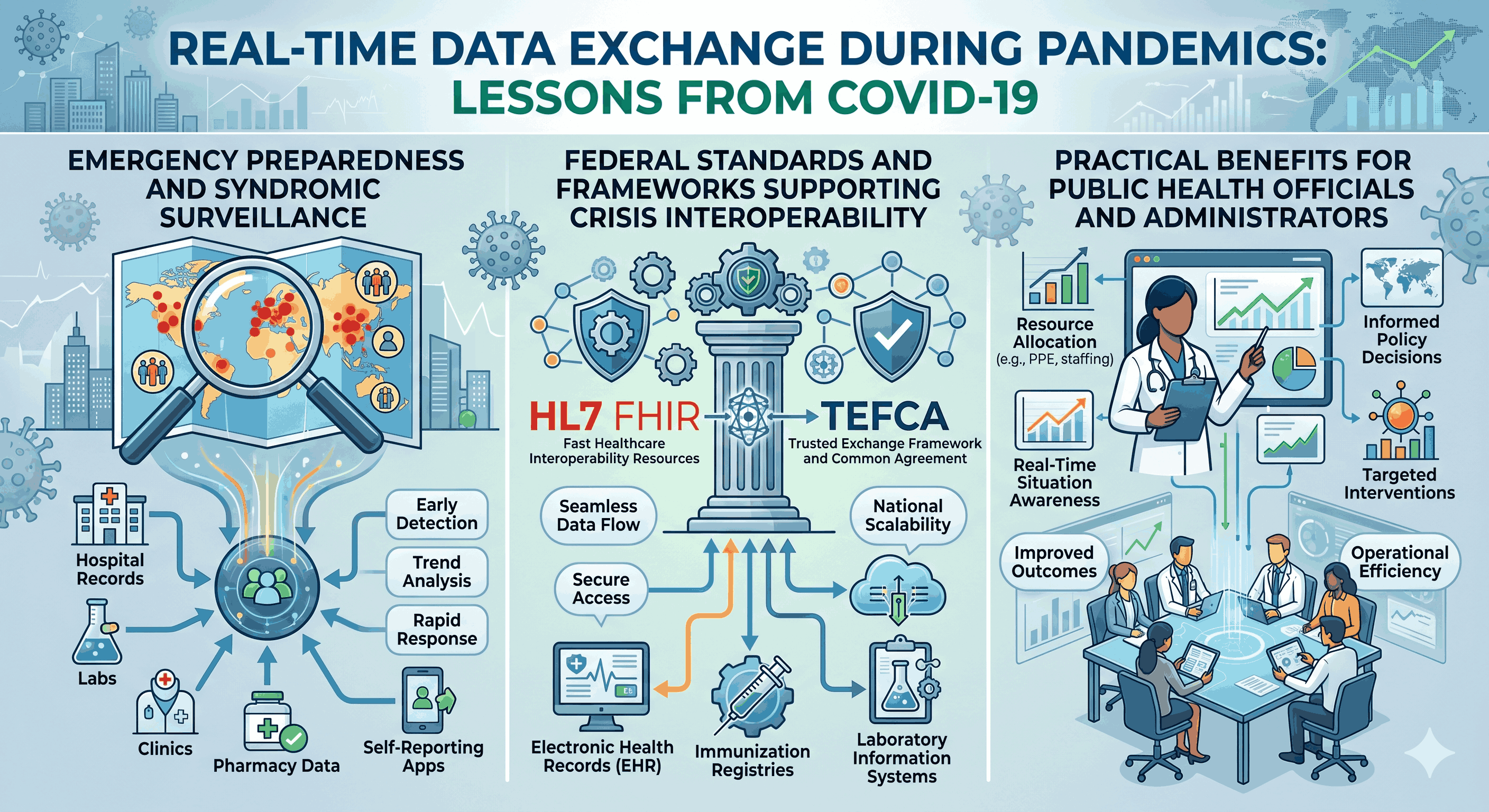
Real-Time Data Exchange During Pandemics: Lessons From COVID-19
COVID-19 stress-tested healthcare data infrastructure nationwide, with mixed results. Some health systems with mature interoperability capabilities adapted quickly. Many others struggled. Key failures included:
- Inconsistent case reporting formats across states, making it difficult for the CDC to compile accurate national data
- Limited electronic case reporting in many settings, forcing reliance on manual processes
- Fragmented lab result delivery, with some test results taking days to reach public health authorities
- Incomplete demographic data attached to test results, limiting the ability to track disparities and target interventions These gaps underscored the need for standardized, real-time data exchange between clinical systems and public health agencies. Organizations that had adopted standards such as HL7 FHIR adapted more effectively than those relying on older protocols. Interoperability is not optional in emergencies. It is foundational infrastructure.
Vaccine Rollout Coordination and Immunization Registries
The COVID-19 vaccine rollout was one of the largest mass immunization campaigns in U.S. history. Coordinating it required real-time data exchange among manufacturers, distributors, clinical sites, pharmacies, and state immunization information systems (IIS). IIS platforms, also known as immunization registries, serve as centralized databases that track vaccine administration at the individual level. All 64 public health jurisdictions in the United States maintain an IIS. These registries depend on accurate, timely submissions from every vaccination site. During the rollout, interoperability gaps created measurable problems:
- Retail pharmacies unable to connect to certain state IIS platforms due to incompatible data formats
- Duplicate patient records when individuals received doses at different locations without a shared identifier
- Difficulty matching first and second doses across separate systems Organizations operating interoperable platforms with pre-built IIS connections experienced fewer disruptions. Near real-time submissions reduced errors and improved dose tracking.
Emergency Preparedness and Syndromic Surveillance
Effective emergency preparedness depends on early threat detection. Syndromic surveillance systems monitor emergency department visits, urgent care encounters, and other clinical data streams to identify unusual patterns that may signal disease outbreaks, bioterrorism events, or environmental hazards.
For syndromic surveillance to function effectively, clinical data must flow automatically from healthcare facilities to public health agencies without manual intervention. Otherwise, gaps emerge, and early warning signals are missed.
The CDC Office of Readiness and Response coordinates national preparedness and response efforts. That coordination is more effective when agencies at every level have access to consistent, current data from hospitals and clinics within their jurisdictions. Interoperability also supports preparedness through:
- Bed availability tracking during patient surges
- Supply chain visibility for medications, ventilators, and PPE
- Patient transfer coordination across facilities using different EHR systems
- Real-time mortality and morbidity reporting to guide resource allocation
Federal Standards and Frameworks Supporting Crisis Interoperability
Several federal initiatives aim to close the interoperability gaps exposed during COVID-19.
TEFCA (Trusted Exchange Framework and Common Agreement)
TEFCA establishes a nationwide framework for exchanging electronic health information under the authority of the 21st Century Cures Act. It creates a common set of rules enabling health information networks to exchange data securely.
Adoption has expanded rapidly. According to ASTP/ONC, nearly 500 million health records had been exchanged through TEFCA as of early 2026, up from approximately 10 million in January 2025. This scale matters during a pandemic, when rapid, trusted access to patient records is critical.
HL7 FHIR (Fast Healthcare Interoperability Resources)
HL7 FHIR is the leading standard for modern health data exchange. It uses APIs to allow systems to request and share specific clinical data.
Unlike batch file transfers, FHIR supports on-demand queries, enabling public health agencies to retrieve relevant records when needed. The ONC Health IT Certification Program now requires certified health IT products to support FHIR-based APIs, accelerating nationwide adoption.
USCDI (United States Core Data for Interoperability)
USCDI defines standardized health data classes and elements required for nationwide interoperability. It functions as a shared vocabulary that allows systems to exchange information consistently.
The draft USCDI v7, released in January 2026, proposes 29 additional data elements to strengthen standardized exchange.
Practical Benefits for Public Health Officials and Administrators
For leaders evaluating interoperability investments, crisis benefits are tangible:
- Faster outbreak detection through automated syndromic surveillance feeds
- More accurate vaccine tracking through real-time IIS reporting
- Improved resource allocation through centralized dashboards reflecting hospital capacity, supply levels, and case counts
- Reduced manual data entry burden during surges
- Stronger health equity analysis through consistent demographic data capture
- Enhanced federal compliance as TEFCA participation and FHIR adoption become baseline expectations Investing in interoperability before a crisis is significantly more effective and less costly than attempting to connect systems during one.
Conclusion
The question is no longer whether interoperability matters during public health emergencies. COVID-19 settled that debate. The question now is how quickly organizations can close remaining gaps.
Public health agencies, hospitals, pharmacies, and EHR vendors all play a role in building the connected infrastructure emergency response requires. Selecting the right integration partner can accelerate that progress.
Iron Bridge Corp has spent nearly 15 years helping healthcare organizations address data integration challenges. With connections to more than 60 immunization information systems nationwide and support for HL7 v2 and FHIR standards, Iron Bridge offers a platform designed for public health preparedness. To learn more, contact a representative.
Frequently Asked Questions
Why is interoperability important during a pandemic?
Interoperability enables hospitals, labs, pharmacies, and public health agencies to share patient data in real time.
During a pandemic, this supports faster case reporting, more accurate contact tracing, and improved coordination of care and resources. Without interoperable systems, organizations rely on manual processes that introduce delays and errors.
How does TEFCA support public health emergency response?
TEFCA provides a nationwide framework that allows health information networks to exchange data under a common set of rules. This enables agencies to securely request and receive patient records across state lines without negotiating separate agreements for each connection.
As of early 2026, nearly 500 million records had been exchanged through TEFCA.
What role do immunization information systems play in vaccine rollouts?
IIS platforms are centralized jurisdictional databases that track vaccine administration. During mass vaccination campaigns, they help monitor coverage rates, identify under-vaccinated populations, manage multi-dose scheduling, and prevent duplicate doses. Their effectiveness depends on timely electronic submissions from all vaccination sites.
What is HL7 FHIR, and why does it matter for emergency preparedness?
HL7 FHIR is a modern data exchange standard that uses APIs to support on-demand clinical data sharing.
Unlike older batch approaches, FHIR enables real-time queries, which are essential when agencies need immediate access to current information. It is now required under the ONC Health IT Certification Program.
How can healthcare organizations prepare for the next public health crisis?
Organizations should assess interoperability gaps and prioritize the adoption of FHIR-based APIs, connection to state immunization registries, TEFCA participation through a qualified health information network, and consistent capture of demographic data. Establishing standards-based infrastructure before a crisis reduces risk and accelerates response.